
You’ve probably seen it at a skin clinic a small device with a bright light that the doctor presses against your mole before making a decision. It doesn’t look like much. But that little tool is one of the most important pieces of equipment a skin doctor uses.
It’s called a dermatoscope, and understanding what it does makes you a much more informed patient.
What Problem Was Dermoscopy Designed to Solve?
When you look at a mole, you see its surface. You can tell if it’s dark or light, roughly what shape it is, and how big it is. But a lot of the features that distinguish a harmless mole from a potentially cancerous one exist below the surface of the skin — in the deeper layers where the pigment cells live.
For most of medical history, doctors had no way to examine those subsurface features without cutting into the skin. The dermatoscope changed that.
By using a combination of magnification and specific types of light — including polarised light that penetrates the skin’s outer layer — a dermatoscope allows a trained clinician to see structures that are completely invisible to the naked eye.
Alt img:”mole screening”
What Makes a Good Dermatoscope?
Not all dermatoscopes are the same. The key factors that determine how useful one is in a clinical setting are:
- Magnification: most clinical dermatoscopes offer 10x magnification, which is the accepted standard for dermoscopic examination
- Lighting technology: cross-polarised light is considered superior for visualising deep skin structures without needing contact gel
- Viewing area: a larger field of view lets the clinician see more of the lesion at once
- Image quality: devices that can connect to smartphones or cameras allow images to be saved and compared over time
- Ergonomics: a tool used dozens of times per day needs to be comfortable and quick to use
A widely used option in Australian clinics is the DermLite DL5 professional dermatoscope it offers 10x magnification, a 32mm viewing area, integrated UV mode, and cross-polarised light technology. It’s also designed to connect wirelessly to a smartphone via the DermLite App, which allows clinicians to capture, annotate, and store patient images during the consultation.
How Does Polarised Light Work in a Dermatoscope?
This is the part that confuses most people, so let’s keep it simple. Ordinary light scatters when it hits the surface of the skin. This creates a glare that obscures the deeper layers — like how sunlight reflecting off water makes it hard to see what’s underneath.
Polarised light oscillates in a single plane. When it hits the skin, the reflected surface glare is filtered out, leaving only the light that has actually penetrated into the deeper layers and bounced back. The result is a clearer, more detailed view of the subsurface structures.
This is why modern polarised dermatoscopes don’t require contact gel and why they’ve largely replaced older non-polarised models in most clinical settings.
What Does the Doctor See That You Can’t?
Here’s what’s actually visible through a dermatoscope that isn’t visible with the naked eye:
- Pigment networks — the mesh-like pattern formed by the distribution of melanin in the skin. Abnormal patterns here are one of the key indicators of melanoma.
- Vascular structures — the patterns formed by tiny blood vessels. Different cancers produce characteristically different vascular patterns.
- Regression zones — pale or grey areas where the body’s immune response has been trying to break down abnormal cells.
- Structural features specific to benign lesions — dermatofibromas, seborrhoeic keratoses, and haemangiomas all have distinctive dermoscopic patterns that help the doctor avoid unnecessary biopsies.
The combination of these features tells a story that the surface appearance alone never could.
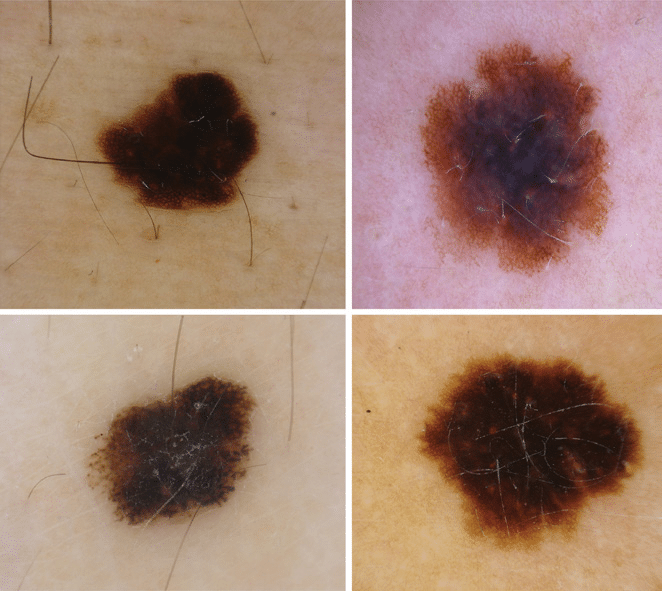
Credit image: Research Gate
Alt text“Examples of dermoscopically and clinically equivocal MSLs from the case study (polarized dermoscopy, 20×) diagnosed histologically. Atypical nevi exhibiting atypical network (A, B), blue-white veil and shiny white streaks (B). Early melanomas (C, D) showing only irregular dots and globules (C) and irregular pigmented blothes (D). Nevi were excised from the abdomen of a 43-year-old woman (A) and the arm of a 51-year-old man (B). Melanomas were excised from the upper back of an 83-year-old man (C) and a 79-year-old woman (D).”
Is Dermoscopy Only for Skin Cancer?
No. While skin cancer detection is its most critical application, dermoscopy is also used for:
- Diagnosing inflammatory skin conditions like lichen planus and psoriasis
- Assessing hair and scalp conditions (a technique called trichoscopy)
- Examining nail disorders
- Evaluating parasitic infections like scabies
A skilled dermatologist uses dermoscopy as a routine part of examining almost any skin condition not just moles.
What Should You Look For in a Skin Clinic?
Not all GPs are trained in dermoscopy, and not all skin clinics have high-quality equipment. If you’re having a skin check, there are a few questions worth asking:
- Do you use a dermatoscope for all mole assessments?
- Is it polarised (which doesn’t need contact gel)?
- Can images be stored and compared at future visits?
A clinician who uses quality dermoscopy equipment and has completed training in its interpretation gives you a significantly better chance of having suspicious lesions identified early.
A Word on Training
It’s worth knowing that dermoscopy is a learned skill. The tool alone doesn’t make the diagnosis the clinician’s ability to interpret what they see does. Studies show that untrained clinicians using a dermatoscope can actually perform worse than experienced clinicians using just their eyes.
This is why professional training and certification in dermoscopy matters. When choosing a skin doctor, look for one who has completed formal dermoscopy training or who works in a dedicated skin cancer clinic.
Alt text:”dermatologist consultation reviewing image on screen”
The Bottom Line
The small device your skin doctor presses against your mole is doing something remarkable — it’s letting them see into your skin in a way that was impossible just a few decades ago. Understanding what it does, and why the quality of that tool matters, makes you a more empowered patient.
If your current doctor doesn’t use dermoscopy, it’s worth asking about — or finding a clinic that does.
| Did you know? |
|---|
| The World Health Organization recognises melanoma as one of the fastest-increasing cancers globally. Dermoscopy, when used by a trained clinician, is one of the most effective non-invasive methods for its early detection. |